microscopic colitis
- related: GI, chronic diarrhea
- patient: older
- pathophysiology:
- sometimes medications such as PPI or NSAIDS
- associated with immune conditions, DM, psoriasis, celiac disease
- sx:
- chronic, watery diarrhea
- dx:
- random colonic mucosal biopsies
- no endoscopically visible inflammation
- subtypes: lymphocytic and collagenous colitis
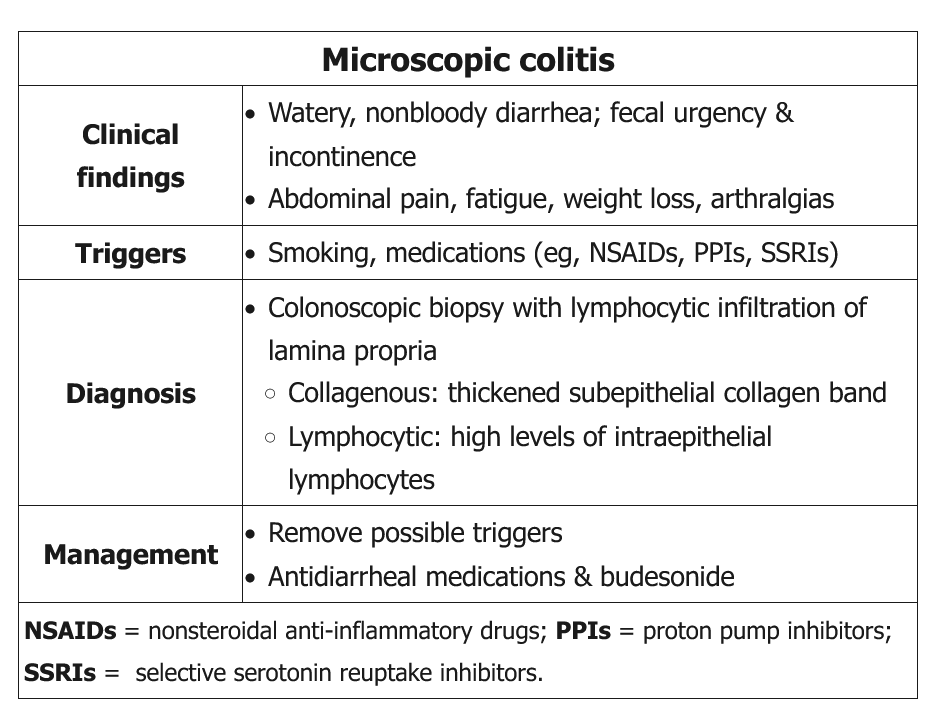
This patient has microscopic colitis (MC), a type of inflammatory bowel disease that disproportionately affects middle-aged women. MC is likely due to an abnormal immune response to various gastrointestinal and external agents, including certain medications (eg, nonsteroidal anti-inflammatory drugs, proton pump inhibitors, sertraline) and smoking. It can be associated with other autoimmune diseases (eg, type 1 diabetes, thyroiditis).
MC presents with chronic watery, nonbloody diarrhea, often with fatigue, weight loss, abdominal pain, arthralgias, or uveitis. The colon appears grossly normal by colonoscopy, but biopsy of the mucosa reveals mononuclear lymphocytic infiltrates in the lamina propria. MC is subdivided histologically into 2 types:
- Collagenous colitis - characterized by a thickened subepithelial collagen band
- Lymphocytic colitis - characterized by high levels of intraepithelial lymphocytes (≥20 for every 100 epithelial cells); focal cryptitis may occur
Initial treatment includes antidiarrheal agents and withdrawal of possible triggering medications. Oral budesonide may be added for active disease or persistent symptoms. Other options for refractory disease include cholestyramine, bismuth subsalicylate, and tumor necrosis factor inhibitors (eg, infliximab, adalimumab).
Tricyclic antidepressants (eg, amitriptyline) are used for moderate to severe irritable bowel syndrome. Irritable bowel syndrome causes chronic abdominal pain and altered bowel habits but would not typically cause weight loss, progressive symptoms, or abnormalities on biopsy.
A gluten-free diet is the therapy of choice for celiac disease, which can manifest as lymphocytic colitis on biopsy; however, this patient has normal IgA levels and absent tissue transglutaminase antibodies, virtually ruling out this disease.
Hydrocortisone suppositories and mesalamine enemas are commonly used in left-sided ulcerative colitis, which is characterized by recurrent episodes of inflammation that are limited to the mucosal layer. Patients typically have bloody diarrhea. Oral mesalamine is sometimes used as a second-line agent in patients with lymphocytic colitis who cannot receive budesonide; however, the benefits are not clear.